Cataract and Femtosecond Laser Assisted Cataract Surgery
If you’ve landed on this page, chances are you have eye-sight issues that are starting to bother you. Congratulations for doing your research! You may be wondering if and how eye lasers can help you get rid of your eye-sight issues. Here there is a break down of the facts behind laser eye surgery for you.Introduction
What is Cataracts and Cataract Surgery?
Cataracts occur when changes in the lens of the eye cause it to become less transparent. This results in cloudy or misty vision. The lens is the crystalline structure that sits just behind your pupil. When light enters your eye, it passes through the cornea (the transparent layer of tissue at the front of the eye) and the lens, which focuses it on the light-sensitive layer of cells at the back of your eye (the retina). Cataracts sometimes start to develop in a person’s lens as they get older, stopping some of the light from reaching the back of the eye. Over time, cataracts become worse and start to affect vision. Eventually, surgery will be needed to remove and replace the affected lens.
Cataract surgery is performed over 400.000 times annually in the UK and millions of happy patients worldwide and is considered by the WHO as the safest surgical procedure of the mankind. Cataract surgery works by exchanging the misty natural and increasingly dysfunctional lens of the eye for a permanent plastic one that depending on it’s type and optical quality can give some form of spectacle independence or just clear distance vision. The general result is a more natural vision for many years to come.
What types of IOLs exist?
RLE employ a wide array of IOLs depending on the patient requirements: level of prescription, the presence of corneal scars, previous eye surgery, pupil size, age of patient, occupation, lifestyle, presence of medical condition like Diabetes, Glaucoma, Macular degeneration etc. Some of the common IOL types are listed below.
- Monofocal: A monofocal lens uses a high precision optic to focus all light passing through the pupil to one focal point, this can be either near or distance or in between depending on Px requirements. (Tecnis ZA, ZCB, Sensar AR40e)
- Multifocal (bifocal, trifocal, sectoral, refractive, diffractive): To be a good candidate you need to already have a significant visual handicap and be a positive person seeing a glass half full as opposed to half empty and do not suffer from diabetes, macular pathologies or states like anxiety, depression, OCD or bipolar. These lenses can be viewed in lay terms as light splitters that some light does the distance and the rest does the near and/or intermediate vision. So, a weak MF lens vs intermediate vs strong lens would split the light to 80-20% vs 75-25% vs 55-45% for distance and near vision respectively. This is the only lens type that induces many images simultaneously and requires a significant brain adaptation that more than 90% of the general population can manage, especially the younger patients. Examples: Tecnis Symfony, ZLB, ZKB, SBL-3, PhysIOL, Zeiss trifocal, Lentis M+ or Mx
- Accommodating: This is the only lens type that tries to utilise the function of the eye as a focusing apparatus. On principle this is a monofocal lens that has the ability due to it’s design to move a bit inside the eye thus improving the depth of focus however, such movement is not sufficient for full spectacle independence and may wean over time. It will require yag laser well before other lens types. Examples: Tetraflex HD (by Lenstec)
- Toric IOL This incorporates a special correction for astigmatism at the top of what is needed for good focus for distance. It can be used on both monofocal and multifocal lenses but not on accommodating lenses
- Monovision or Blended vision: This is not a lens but a method of using monofocal lenses to increase depth of focus. Around 50% of the general population can tolerate a moderate imbalance of focus between the two eyes (Rx imbalance of -1.50D) when one eye doing near vision and the other distance and almost 95% can tolerate a relative imbalance with a mini-monovision (Rx imbalance of -0.75). This results in some imbalance and impaired 3D perception but improves functional spectacle independence in a natural way without the introduction of many aberration and glare and can easily be enhanced for better near or distance by the use of special spectacles.
- Piggy-bag IOL (Sulcoflex): This is a plane simple monofocal or multifocal lens like a contact lens very thin and elastic used to correct refractive surprise or to introduce mutlifocality after an otherwise successful cataract RLE surgery or a monofocal lens.
- Aphakic (Artisan): This is an Iris haptic IOL (iris claw) very much like the p-IOLs however much thicker and placed behind the pupil. It is used exclusively for Px that had a complicated cataract surgery
Am i a Good Candidate for Cataract Surgery?
If you are experiencing increasingly blurry vision, increased glare at nigh, changing eyeglasses every year or even glasses cannot help you see clearly for the majority of your activities then yes you could be. The procedure is generally safe for all eye types though patients with denser, white cataracts or higher prescriptions should take precaution.
How it Works to Get Younger Vision?
IOLs through a cataract surgery refresh and rejuvenate the vision by removing an ageing dysfunctional lens and replacing it with a clear more optically perfect lens thus turning back the clock. The majority of over 70s feel that their vision is like it was on their 40s.
How many Treatments will You Need?
Usually one but if you have a refractive surprise (5-10%) then you will likely need an enhancement with wither LVC or piggybag lens. It is likely (5% per year) that you will need yag laser posterior capsulotomy to clear the skin that contains the lens, this will not need to be repeated, it is minimally invasive and you can return back to work a few hours later. Additionally, if you had a multifocal lens and failed to adapt to its’ side-effects (0.5%) then you may need to exchange your IOL to a weaker multifocal lens or to a monofocal.
What are The Benefits of This Treatment?
Improvement of visual clarity both definition and quality, along with some minimisation of spectacle dependance for the majority of the activities

Does This Treatment Cause Any Harmful Effects?
According to most studies anything from 1 to 10% of patients with multifocal lenses may experience adverse effects. Side effects include temporary discomfort, redness and swelling. Without proper attention the eye may become inflamed and infected. No long-term effects are directly and exclusively associated with lens surgery however, dry eyes, floaters, glare, edge effects haloes, starbursts and ghosting may affect a minority of patients (less than 1%) for more than the usual month or two say over 6-12 months. More serious but rare events include retinal detachment (1/5.000), CME, ERM, macular hole, infection (1/10.000), loss of sight, loss of the eye-globe (1/100.000)
What Patients Have Experienced?
People who have availed of IOL surgery report a very low level dull ache starting hours after the treatment which may last for the night. A sharp pain may happen if there is a corneal abrasion but that is unusual. Those who have availed of IOL surgery for cataract noticed dramatic and more visible results a day after treatment, while those who chose the implantation of multifocal IOLs they are impressed with the improvement of their near vision.
Bottom Line
As you continue your search for the ultimate solution to your visual problem, remember that there is no one procedure that can solve all your eye care worries in a single treatment and there are side-effects that can be irreversible. If you have a cataract then this surgery is not elective you have to do it however, the choice of IOL is elective and need to think carefully under my guidance what is best for your needs.
Special Considerations:
1. Cornea Guttata, Depleted Corneal Endothelial Cells or Fuch’s Corneal Endothelial Dystrophy.
The corneal endothelium is the base layer of cells lining the inside of the cornea (see images under corneal transplant). These cells are responsible for maintaining corneal transparency and clarity. We are born with a certain number of these cells that gradually decline with age (at a rate of less than 1% per year) as they are not renewable and may vary between different individuals.
This number (concentration of cells) is important when considering any elective corneal or lens surgery as some of these cells are expected to be damaged. Corneal function and clarity can be maintained even if the cell count is very low (1000) however, there is a critical level below which (500-600) the cornea will start to cloudy over due to water-logging. If that was to happen then special medicine drops will need to be used and even surgical options like DSEK may need to be considered (read under corneal transplant).
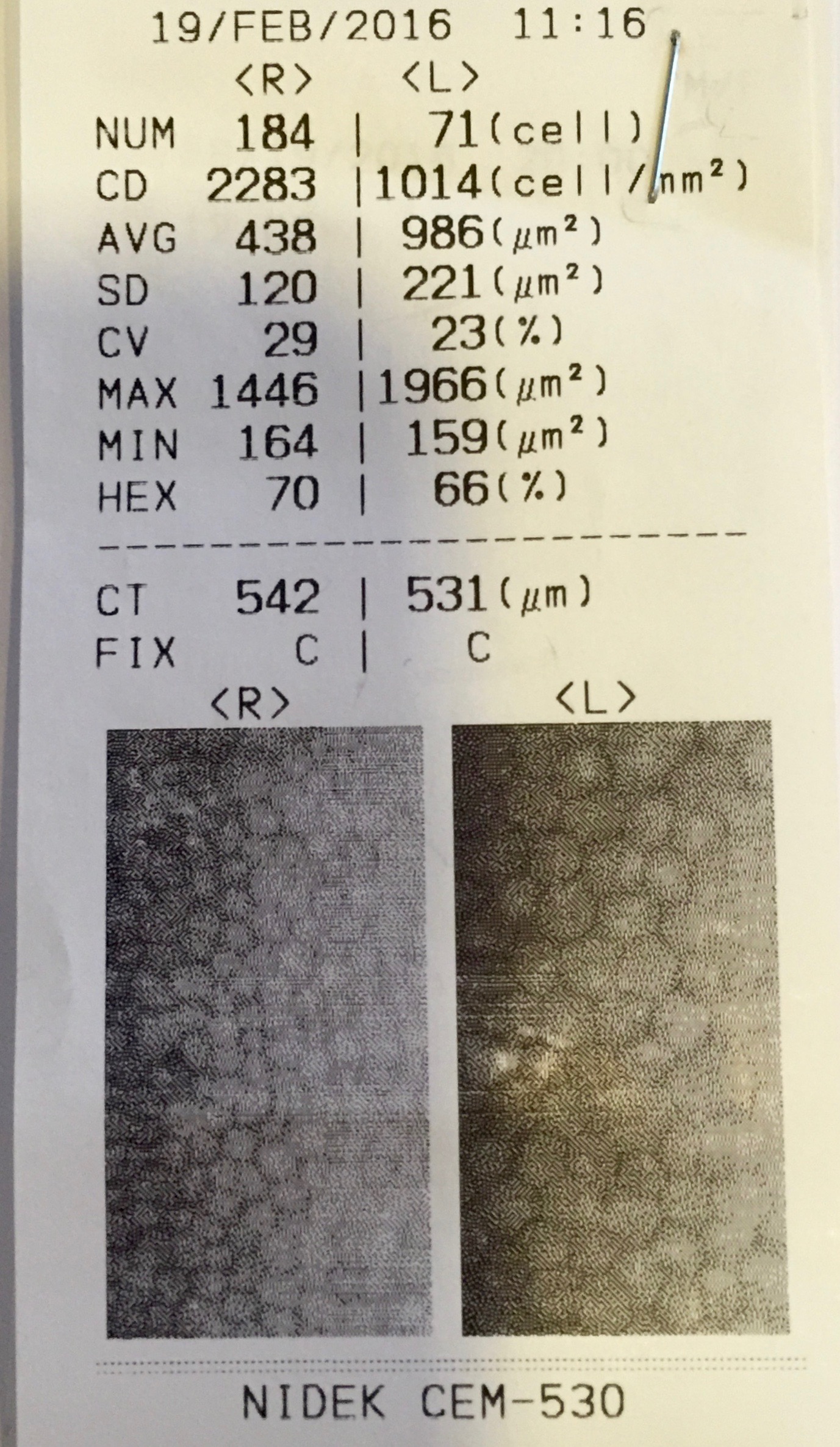
These cells are measured routinely in all patients seeking cataract or lens surgery with a special camera instrument (specular microscopy). This measures the number/density/size/shape/volume of those cells as per image below: Here you can see a rather normal density of cell with small size hexagonal cells on the right eye (left of the picture) whereas the left eye (right of picture) has half the number of cells, which are double in size to compensate for the deficit.
2. Keratoconus and Cataract:
The keratoconus typically induces loss of vision through abnormalities in the corneal shape. When this is compounded with a further visual loss from the development of cataract it presents a challenge in selecting the correct IOL type, power and in the operation. Below is a patient with regular astigmatism and moderate cataract.
More information
Who is cataract surgery suitable for
What is the recovery time?
Book Your Consultation
Please book your consultation online by clicking the enquire now button below and filling in your details. Our team will get back to you as soon as possible.